Problem Statement
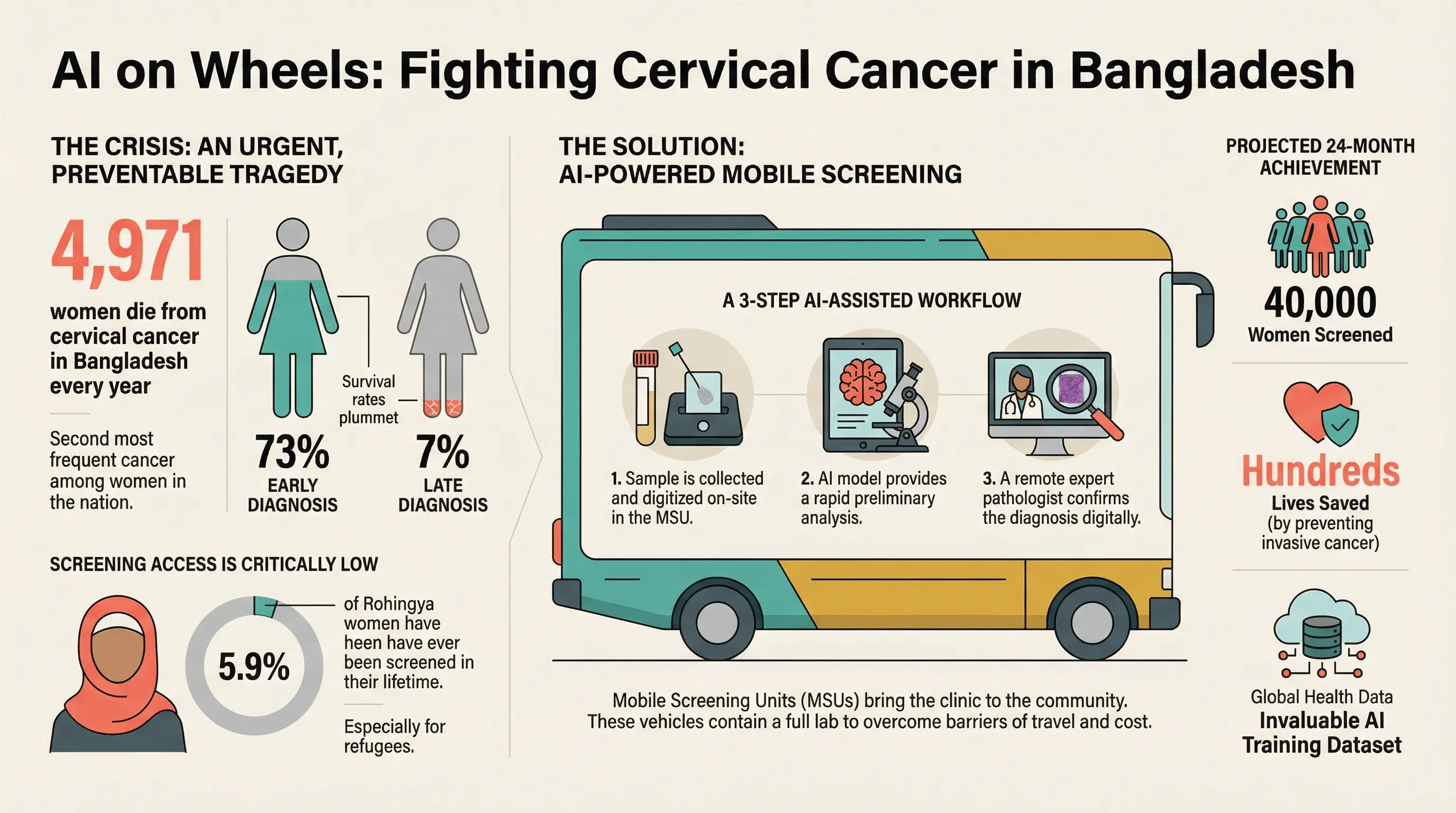
Cervical cancer represents a significant and preventable public health crisis in Bangladesh. It is the second most frequent cancer among women nationwide, with current estimates indicating that 8,268 women are diagnosed and 4,971 die from the disease every year. This high mortality is a direct consequence of late-stage diagnosis, a reality underscored by the fact that five-year survival rates plummet from 73.2% for early, localized cancers to a devastating 7.4% for advanced-stage disease.
The core of the problem lies in the profound lack of access and availability to screening. National screening coverage for women aged 30-49 within a five-year period is critically low at approximately 5%. This gap is catastrophically wider in marginalized communities. Among more than one million Rohingya refugees in Cox's Bazar and Bhasan Char, a population with a deep-seated mistrust of formal healthcare systems, studies have found that as few as 5.9% of women have ever been screened in their lifetime. This is compounded by a high prevalence of risk factors and a severe lack of awareness; in one assessment, only 11.8% of Rohingya women had even heard of cervical cancer.
Solution
NoeticX is proposing Project Surokkha, a plan to deploy a revolutionary AI-powered mobile screening ecosystem. This initiative is engineered to dismantle the systemic barriers of access, cost, cultural mistrust, and the scarcity of specialist clinicians and pathologists.
The cornerstone of Project Surokkha's implementation strategy is the Mobile Screening Unit (MSU), a self-contained clinical and laboratory environment built into a vehicle. This portable solution is the key to overcoming the primary barrier of physical access to healthcare facilities. Instead of requiring women to travel, the MSU brings the entire screening and diagnostic workflow to their community.
Target Population
The project will focus on the Rohingya refugee camps in Cox's Bazar and Bhasan Char, as well as the host community of Cox's Bazar. Based on a recent survey by UNFPA in 2024, there are 247,006 women of reproductive age among the Rohingya population. Phase 1 aims to screen 15,000 reproductive-age women (aged 30-60). Phase 2 will expand to include an additional 25,000 women from the camps and the surrounding underserved host communities.
Key Objectives
- To screen a total of 40,000 women over a 24-month period.
- To achieve a screening coverage of at least 15% within the targeted camp clusters, drastically exceeding the national average.
- To provide immediate visual results, enabling quick decisions on subsequent diagnostic procedures and treatment interventions.
- To establish and ensure a seamless, fully managed referral pathway for diagnosis and treatment for all women identified with precancerous or cancerous lesions.
- To validate a cost-effective, scalable, and replicable model for cervical cancer screening that can be deployed in other low-resource and humanitarian settings globally.
- To build sustainable local capacity by training a dedicated cadre of Rohingya Community Health Workers and Bangladeshi medical technologists in advanced screening techniques.
Technical Architecture & Implementation Workflow
The cornerstone of Project Surokkha's implementation strategy is the Mobile Screening Unit (MSU), a self-contained clinical and laboratory environment built into a vehicle. This portable solution is the key to overcoming the primary barrier of physical access to healthcare facilities. Instead of requiring women to travel, the MSU brings the entire screening and diagnostic workflow to their community.
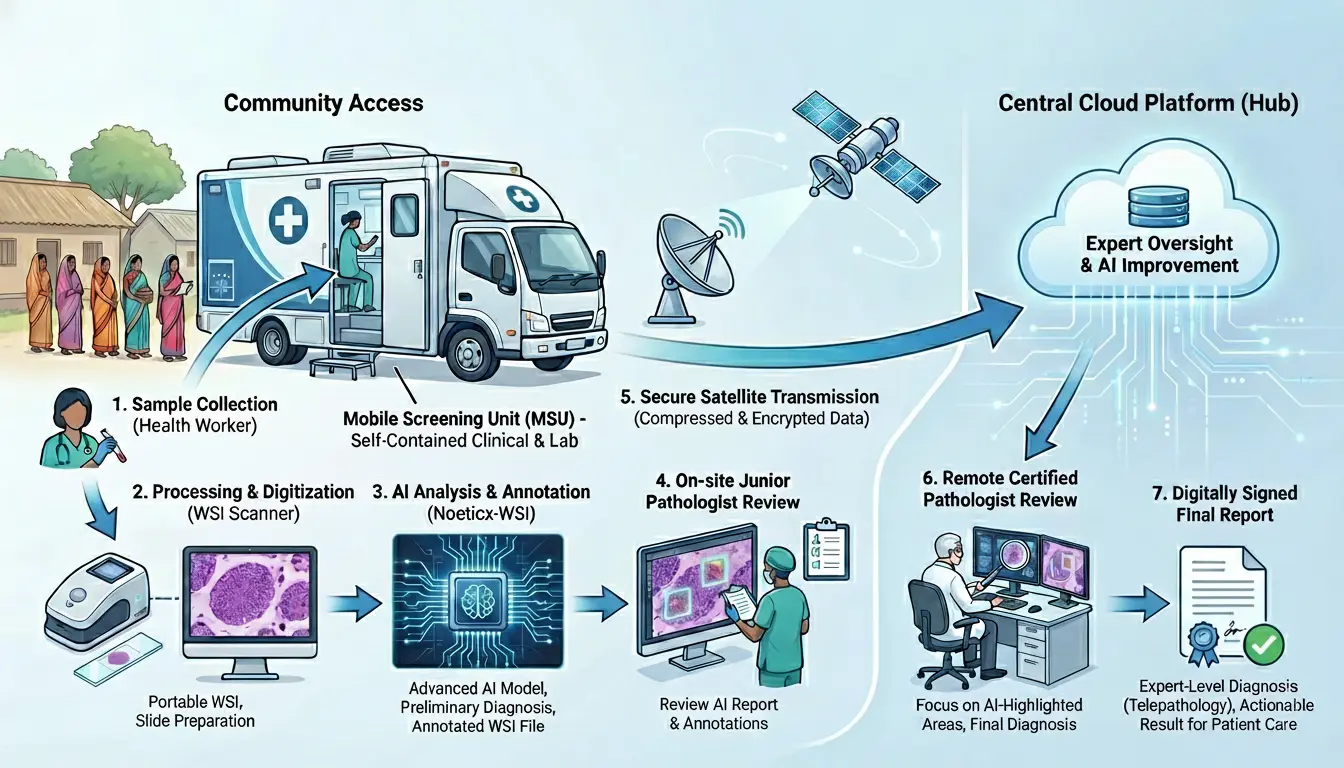
Figure: Hub-and-Spoke Operational Model - From Community Access to Central Cloud Platform
Project Surokkha utilizes a hub-and-spoke operational model. The "spokes" consist of three MSUs that deliver care at the point of need. The "hub" is a central cloud-based platform for expert oversight and continuous AI model improvement.
A trained health worker will collect cervical fluid for conducting PAP smear. The sample is processed and digitized within the MSU using a portable Whole Slide Imaging (WSI) scanner. An advanced AI model, Noeticx-WSI, performs a detailed analysis of the digital slide, and generates an annotated WSI file and a preliminary diagnosis for an on-site junior pathologist. This annotated WSI file, along with the AI-generated report, is compressed and securely transmitted via a satellite internet connection to a remote, certified pathologist. The pathologist reviews the AI's findings, focusing their attention on the highlighted areas of interest, makes the final diagnosis, and digitally signs the final report. This telepathology workflow enables expert-level diagnosis without the expert ever needing to be physically present.
Quantifiable Achievements (24-Month Targets)
| Metric | Projected Achievement | Significance |
|---|---|---|
| Women Screened | 40,000 | Providing life-saving preventive care to a large, previously unreached population. |
| Lives Saved | Hundreds | By detecting precancerous lesions early, the project will prevent hundreds of women from developing invasive cancer, where survival rates can be as low as 7.4% for advanced stages. |
| Data for Global Health | Invaluable Dataset | Creation of one of the largest, ethically sourced datasets of cervical imagery from a vulnerable population, crucial for training less biased and more robust AI models for global use. |
Conclusion
Project Surokkha is designed to deliver a transformative impact on women's health in Bangladesh by directly addressing the root causes of high cervical cancer mortality. By deploying a mobile, AI-powered screening ecosystem, the project directly confronts the challenges of geographic inaccessibility, the severe shortage of specialist pathologists, and the cultural obstacles that prevent women from seeking care.